








Everything You've Ever Wondered About the Placenta
everything you've ever wondered about the placenta
Written by Jade | Midwife, Mama of 3 & Tiny Hearts Educator
The placenta; what a beautiful structure!
To start off, here are some amazing facts about the placenta:
✨It's the only organ you're not born with.
✨It's the only organ you grow during pregnancy.
✨ The placenta weighs around 700g at the end of pregnancy.
✨It helps to grow our bubs.
✨It provides unborn bubs with oxygen and nutrients they need from a mama's body.
✨Deoxygenated blood and waste products go from bub's body back to the placenta.
✨The average placenta is around 22cm in diameter.
✨Certain medications and infections can cross the placenta and be passed to bub.
✨ It takes around 4-6 weeks for the wound where the placenta was attached to the inside of your uterus to heal.
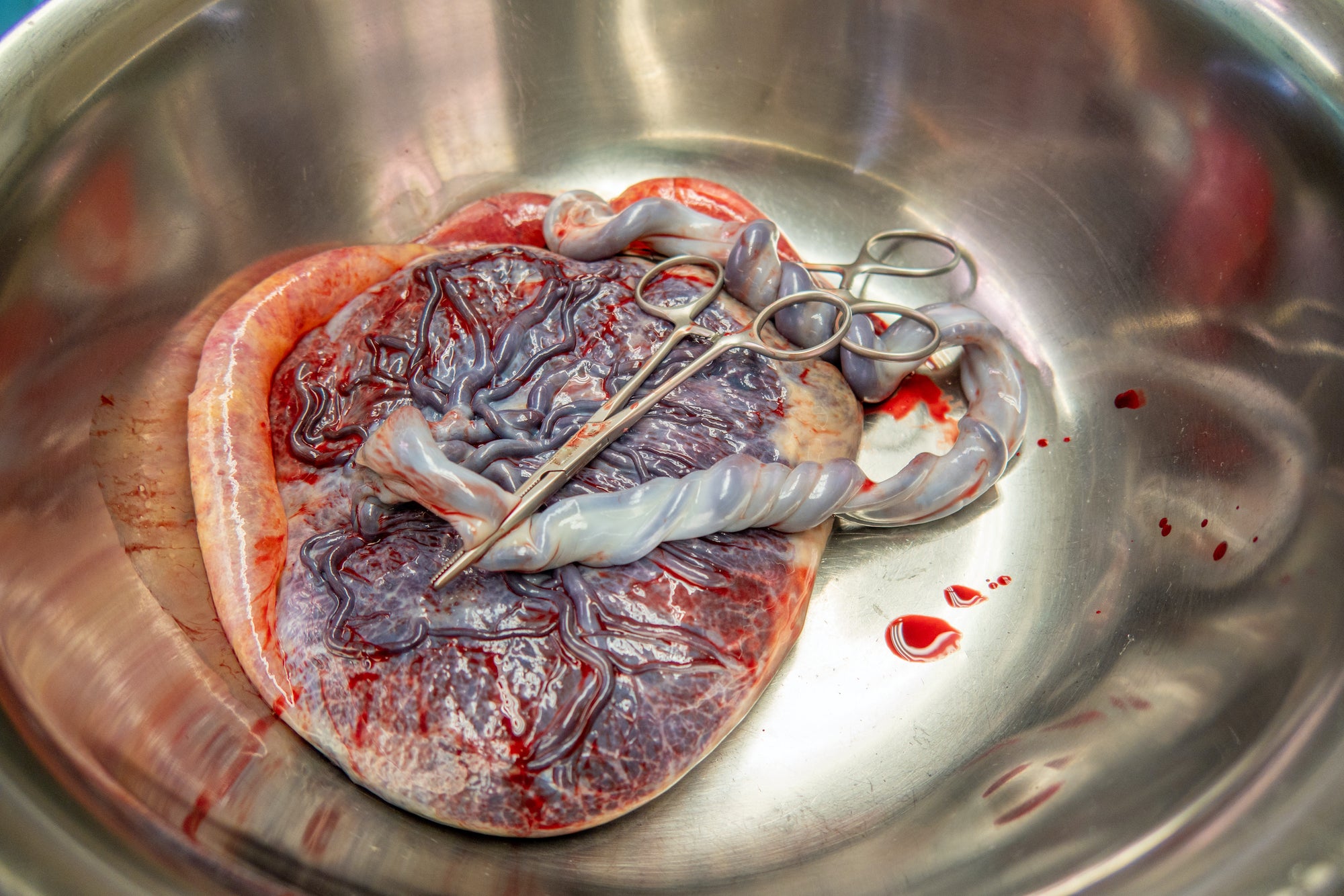
anatomy of the placenta
The meaty side of the placenta sits outside the sac, and is attached to a mama's uterus. Bub grows inside the sac, which is fully sealed all around them until a hole is created and a mama leaks fluid [the waters break]. There is also a cord attached from bub's belly button area to the placenta. The meaty side of the placenta is made up of little parts called cotyledons and is full of blood vessels. The sac is made up of two layers- the amnion and the chorion.
anatomy of the umbilical cord
The umbilical cord is made up of two arteries and one vein. The umbilical vein carries highly oxygenated blood from the placenta to bub, while the two arteries carry blood with low oxygen levels back to the placenta.
The jelly-like substance around the cord is called Wharton's Jelly. Wharton's Jelly helps protect the cord from things like cord compression and true knots, which can impact the blood flow to and from bub. Wharton's Jelly is particularly important during labour and birth because everything can become compressed during contractions and while pushing.
While some sources vary, the average length of an umbilical cord is said to be between 50-60cm. Some bubs have a short cord, and others have an extra-long cord. In fact, a 2012 study showed a huge variety of cord lengths, with the shortest umbilical cord being 24cm and the longest being 124cm [1.24m!!]. The study also showed that bubs with short and long cords were more likely to have complications such as abnormalities in bub's heart rate during labour, but the length isn't related to bub's gender, weight or length.
If bub is born with a short cord, they may be placed on your belly rather than your chest immediately after birth until the cord is cut and clamped. That's because on the other end of the cord is the placenta, which may still be attached to your uterus.
delivery of the placenta
The third stage of labour starts with the birth of your bub and ends with the delivery of the placenta. During the third stage, you may feel vaginal pressure again as the placenta moves down. However, it may not be as intense as during the second stage [bub being born]. You will continue to feel contractions during this stage, as the contractions are now working to expel the placenta from the uterus

variations of the placenta
The umbilical cord is attached in the middle of a normal placenta, and it's one big piece. These are some of the other variations that can occur in a placenta:
Battledore cord insertion
When the cord is attached somewhere around the edge of the placenta.
Velamentous cord insertion
When the cord travels through the amniotic sac [potentially not protected by Wharton's Jelly] to insert into the very edge of the placenta.
Placenta fenestrata
When the middle part of the placental tissue is thin or absent.
Bipartite placenta
[Also known as bilobed placenta] is when a placenta is separated into two equal-sized lobes. The placenta can also be split into many equal-sized lobes, and this is named according to how many lobes are present, e.g. three lobes= trilobed. If the pieces aren't equal and one is smaller, this is called a succenturiate lobe.
Succenturiate lobe
When the placenta has an extra piece that's separate from the main part of the placenta. You can have one or more succenturiate lobes.
Circumvallate placenta
When the amniotic sac pieces double back on themselves, creating a ring around the surface of the placenta.
Where placentas attach within the uterus can also differ.
placenta positions
During pregnancy, the placenta may be embedded in a number of different places inside the uterus. Some of those places include:
Anterior position
An anterior placenta means your placenta is attached to the front of your tummy, and bub is behind. It can mean you feel movements a bit later in pregnancy but is otherwise a normal place for your placenta to develop. You should still feel movements and continue to monitor and know bub's normal pattern from around 28 weeks onwards.
Posterior position
A posterior placenta means your placenta is attached to the back of your tummy, and bub sits in front. A posterior placenta might help you feel bub's movements a bit earlier, and similar to an anterior placenta, it is otherwise normal.
Fundal position
A fundal placenta means your placenta has embedded into the top of your uterus called the fundus, and bub will swim around underneath. When delivering the placenta, your healthcare team will take extra care to make sure the placenta has separated before pulling on the cord to help deliver it. Otherwise, no concerns here either.
Low lying/ Previa
If your placenta is close to, touching or completely covering the os [the cervical hole that opens up for bub to exit vaginally], it's considered low lying or a Previa. If this is found at your 20-week scan, you'll be rescanned around 32 weeks to check it has moved upwards, which most will do, and closely monitored for bleeding. There are four grades of a placenta previa depending on how close or how much of the os it covers.
en caul birth
In some births, bub may be born still inside their amniotic sac. This means your waters won't break, and instead, bub will come out still swimming around in them. When this happens, bub is said to be born 'en caul' or in other words, still inside the amniotic sac at birth. If your bub is born en caul, your health care team will 'pop' your amniotic sac to remove the amniotic sac from around bub shortly after birth. Only around one in every 80,000 bubs are born en caul.
lotus birth
Lotus birth is when a cord is NOT cut or clamped and remains attached to bub after birth. The placenta and cord are left to detach from bub's belly itself, which usually occurs around 5-15 days after birth [however, some sources say it takes between 3-10 days, while others say 7-10 days].
Once the placenta is birthed, it's usually washed in warm water using a sieve by a mama and papa-bear and rubbed with salt and herbs to help dry it out, prevent it from becoming smelly and slow the growth of bacteria. It's then wrapped in clean dressings and put into a cotton bag or swaddled with bub until it naturally separates.
It came about in the 1970s from Clair Lotus Day, who decided to have a lotus birth after becoming aware that chimpanzees didn't always remove the placenta from bub after birth.
There's limited to no quality research into the benefits and risks of lotus birth, so this is something to discuss before going into labour with your chosen healthcare provider. Because of the lack of research, the Vic Government advises that it's not currently a recommended practice.
If you choose to have a lotus birth, it's really important to monitor bub for signs of infection, particularly at their umbilical stump. You're looking for redness, a funny smell, or discoloured discharge around the stump itself, a fever, or bub behaving differently [such as poor feeding, reduced output, lethargic etc].
delayed cord clamping
Delayed cord clamping is when the umbilical cord is not clamped or cut until after cord pulsations have stopped or around 1-3 minutes after birth. Some mamas choose to not cut or clamp the cord until after the placenta is delivered. When doing delayed cord clamping, you may see the cord go pale, limp and white as all of the blood has left the cord, like you can see in the image above.
In most birth suites, this has become a standard part of the birthing process unless there is a medical reason that the cord needs to be cut immediately [e.g. your bub needs resuscitation].
Delayed cord clamping is said to increase iron stores for bub, as well as haemoglobin levels [a blood cell that carries oxygen] and blood volume. It has even more benefits for preterm bubs. However, small studies have shown that delaying cord clamping increases the risk of jaundice. It's important to know that if you're planning to collect stem cells from the cord for umbilical cord blood banking, you're not able to have delayed cord clamping, as the cord must be clamped and cut early to maximise the amount of stem cells collected.
If this is something that you'd like as part of your birth journey - make sure you discuss it with your midwife or doctor before the big day as part of your birth plan.

what can you do with your placenta after birth?
Placenta encapsulation
Placenta encapsulation is when a mamas placenta is dehydrated, broken down and put into capsules for her to take orally. Some mamas do this because it's said to improve your milk supply, mood and iron stores while decreasing your chance of postpartum depression and baby blues, but a lot more research is needed in this area to support these claims.
Use it to create an art work
The placenta is often referred to as 'the tree of life'. You can lay your placenta down flat, with the shiny side facing up and the cord pointing down. Lay a piece of paper or cardboard against the shiny side of the placenta and press firmly. The blood vessels on the back of the placenta will press against the paper. Gently peel the paper back, and in the artwork, you'll see something that resembles a tree of life.
Eat it
Some mamas choose to eat their placenta after birth. There's minimal research on this, though, so I'd strongly encourage you to chat with your healthcare providers before choosing to take it home and eat it.
Bury it and plant a tree over it
This one is practised by many cultures but is gaining popularity amongst mamas and papa-bears here in Australia too. You take the placenta home, dig a hole [that is deep so that animals won't dig it up], put the placenta in and place some dirt on top, plant a new tree over it, and watch it grow.
There are certain conditions that may impact the placenta:
placneta acreta, increata + percreta
Accreta
A placenta accreta is when the placenta grows onto the muscle layer of the uterus.
Increta
A placenta increta is when the placenta grows into the uterine muscle.
Percreta
If a placenta grows all the way through the uterus and into other organs, like the bladder and bowel, it's considered a placenta percreta.
retained placenta
A retained placenta is when the placenta hasn't been delivered after a specific amount of time, depending on the type of third stage you're having. That amount of time is 30 minutes if you decided on an active third stage [when you have an injection of Oxytocin into your leg shortly after birth]. However, that time changes to 60 minutes if you decided against the Oxytocin injection and instead opted to try other methods, like skin to skin and breastfeeding, to promote natural Oxytocin, which is called a physiological third stage.
Once bub is born, your Doctor or Midwife will look for signs that the placenta is separating from the uterus in order to be birthed, such as a trickle of blood and lengthening of the cord. You might also feel more contractions. Once those signs are there, you've got two options [but can't do them simultaneously]:
1: A Midwife or Doctor will gently place traction on the cord to help deliver the placenta.
2: You'll push to birth the placenta.
In both of these scenarios, your Doctor or Midwife will place their hand near your uterus to 'guard' it [stop it inverting or coming out, which is very rare].
If the placenta isn't coming, you could try position changes, doing a wee or reinserting the catheter if you had an epidural or can't get up to empty the bladder, breastfeeding bub, skin to skin and attempting to push the placenta out yourself. If these are still not working and you're sneaking towards those recommended time limits or losing a lot of blood, your Doctor may recommend going to theatre and being put under general anaesthetic to manually remove the placenta.
Retained placenta can be caused by your cervix closing before the placenta has been delivered, ineffective or absent contractions or a placenta that isn't separating from your uterus for whatever reason.
In some cases, a small amount can be retained and may not show up until later when a mama has a fever, pain, smelly/ discoloured vaginal discharge, a big bleed or is losing clots.
placental abruption
Placental abruption is the most common cause of bleeding during the second half of pregnancy. It happens during pregnancy or labour when some or all of the placenta comes away from the uterine wall. It occurs in around 1% of pregnant mamas in Australia with almost half occurring after 37 weeks.
Trauma, such as falling onto your bump or a car accident, may cause a placenta abruption, but sometimes the cause is unknown. What we do know is that some risk factors may increase the risk of having an abruption:
- A previous placenta abruption
- Breaking your waters preterm or having more waters than normal [polyhydramnios]
- Twin/ triplet pregnancy
- Smoking
- Drug use
- High blood pressure
- Pre-eclampsia
- Infection
- Aged 35+
- Performing an ECV [occurs in less than 1% of ECVs]
The symptoms for placenta abruption are different for everyone, but generally, most women experience:
- Constant abdominal pain, which may be mild or severe in the tummy or back.
-Bleeding. Most mamas will bleed with an abruption, but the amount of blood doesn't indicate how severe the abruption is. Some mamas won't lose any blood because some [or all of] the blood may be trapped behind the placenta.
If you think you're having a placental abruption, you need to immediately contact your pregnancy care team. You'll be invited in to monitor you and bub with a CTG, ultrasound and speculum to check where the bleeding is coming from and watch for any further bleeding or signs of distress. If you experience sudden, severe abdominal pain and heavy bleeding, call 000 for an ambulance. [Don't forget, you don't have to lose blood to be having an abruption].
Your placenta is your bub's oxygen source, meaning a placental abruption can be a life-threatening emergency, depending on how much has abrupted. Some mamas who have had a partial abruption, with the right pregnancy care, can continue on to have a full-term pregnancy. Other mamas will need bub to be born immediately. Your birthing team will have that discussion with you.
I hope that clears up some of the confusion or uncertainty you had around placentas. If you've got any more questions, feel free to leave them on the original post on Instagram or Facebook. Tag your tribe + let me know in the comments, what amazes you the most about placentas? 💗
bump, birth and beyond
$350
The Bump, Birth & Beyond course will educate you and your co-pilot (support person) on what to expect during pregnancy, birth and the first trimester with your new little love.

To the extent permitted by law, Tiny Hearts excludes any liability, including any liability for negligence, for any loss, including indirect or consequential damages arising from or in relation to the use of this blog content.
This blog may include material from third party authors or suppliers. Tiny Hearts is not responsible for examining or evaluating the content or accuracy of the third-party material and it does not warrant and, to the fullest extent permitted by law, will not have any liability or responsibility for any third-party material. This blog was written for informational purposes only and is not a substitute for professional medical advice. Nothing contained in this blog should be construed as medical advice or diagnosis.The content on our blog should not be interpreted as a substitute for physician consultation, evaluation, or treatment. Do not disregard the advice of a medical professional or delay seeking attention based on the content of this blog. If you believe someone needs medical assistance, do not delay seeking it. In case of emergency, contact your doctor, visit the nearest emergency department, or call Triple Zero (000) immediately.
The author of this information has made a considerable effort to ensure the information is in-line with current guidelines, codes and accepted clinical evidence at time of writing, is up-to-date at time of publication and relevant to Australian readers.